How do we treat autoimmune encephalitis?
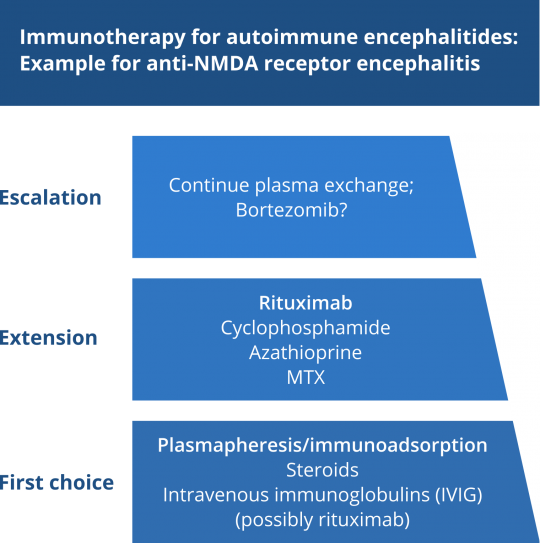
At present, there are no prospective clinical trials, but only good retrospective therapeutic data on anti-NMDAR encephalitis. Therefore, the therapy of the autoimmune types of encephalitides is oriented on the therapy established for anti-NMDAR encephalitis (Figure). When rapid-onset immunotherapy is given, the prognosis is not only principally good for anti-NMDAR encephalitis, but also for other encephalitides with antibodies against neuronal surface proteins. That is why any delays in treatment initiation should be minimized.
The following principles apply: The therapy of paraneoplastic and non-paraneoplastic autoimmune encephalitides in which antibodies against intracellular and membrane-based neuronal antigens are demonstrated should consist of a combination of
- Adequate cancer therapy (surgery, radiation chemotherapy), provided a tumor can be detected
- Immunotherapy and
- Symptomatic therapy.
According to experts’ opinion, the following immunosuppressant dosage and interval regimens are mostly used:
First-line therapy:
- Plasmapheresis/immunoadsorption (5-10 cycles)
- Intravenous immunoglobulins (2 g/kg body weight for 5 days)
- Intravenous methylprednisolone pulse therapy (1 g/day for 5 days)
Second-line therapy:
- Rituximab (1000 mg i.v. twice at 14-day intervals, repeat after 6 months as needed) → innumerable experts meanwhile give rituximab as first-line therapy, underpinned by its comparatively favorable side effect profile and its relatively selective action on the depletion of B cells
- Cyclophosphamide for 6-12 months at a dose of 750-1000 mg/m² body surface area i.v. every 4 weeks with dose escalation as a function of leukocyte nadir
- Azathioprine (100-250 mg/day)
- MTX (7.5-25 mg/week), folic acid rescue
Some specialists recommend a second-line therapy (including a combination of enhancement therapy drugs, e.g. rituximab together with cyclophosphamide) after as early as 10-14 days of no response (Dalmau 2011). In therapy-refractory patients, more recent observations suggest a positive effect of bortezomib, the proteasome inhibitor used to deplete mainly mature plasma cells (Scheibe et al.).
References
- Dalmau J, Lancaster E, Martinez-Hernandez E, et al. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurol 2011;10(1):63–74.
- Scheibe F, Prüss H, Mengel AM, Kohler S, Nümann A, Köhnlein M, Ruprecht K, Alexander T, Hiepe F, Meisel A. Bortezomib for treatment of therapy-refractory anti-NMDA receptor encephalitis. Neurology. 2017 Jan 24;88(4):366-370.